
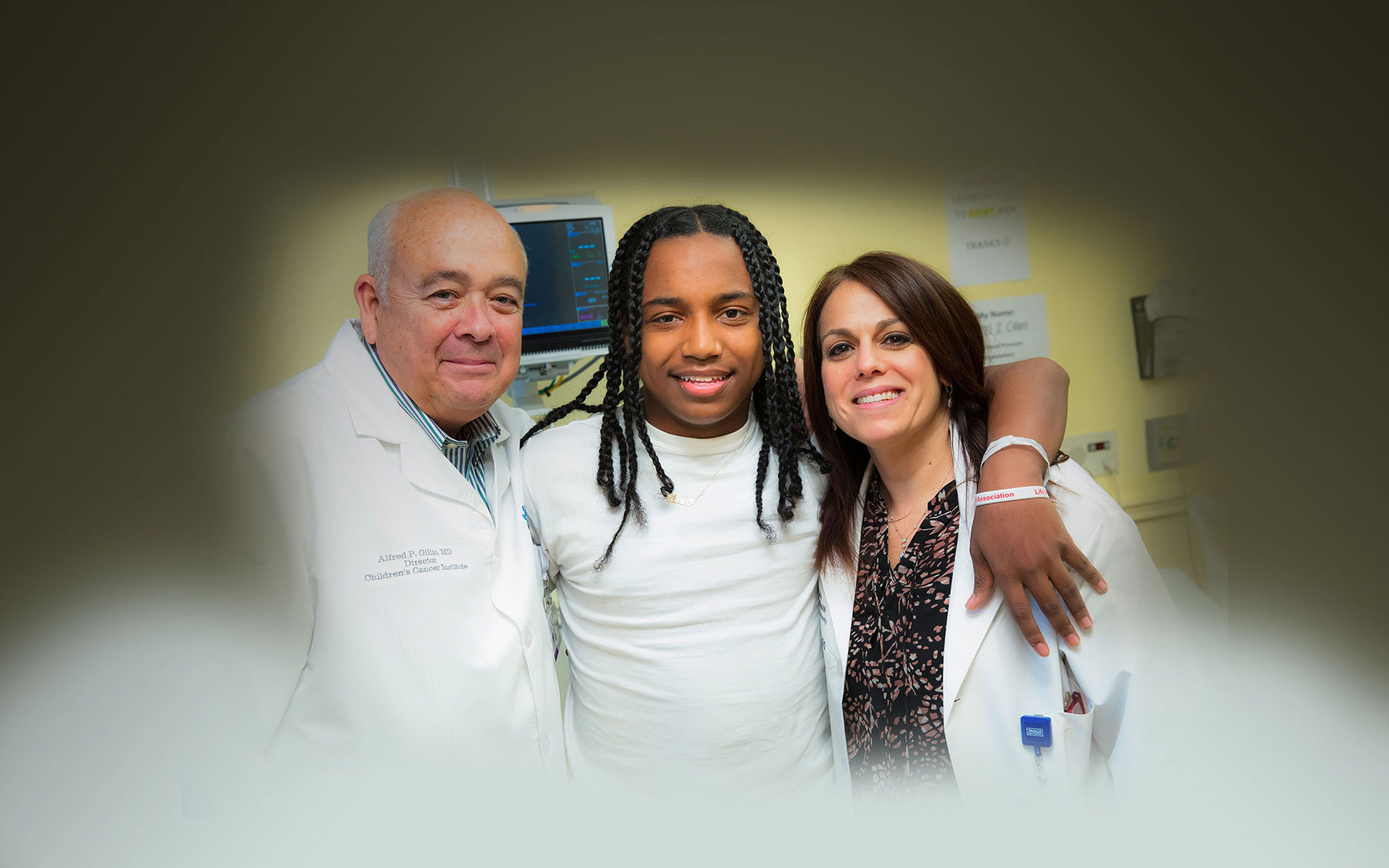
Meet Razel
For 18-year-old Razel Colón of Hoboken, New Jersey, not all childhood memories are warm and fuzzy. That’s because Razel didn’t have a normal childhood. Instead of sports, swimming pools, sprinklers and sleepovers—things most kids enjoy and take for granted—he remembers wheelchairs, IVs, heating pads and hospital beds. And pain. Excruciating, debilitating pain.
“I have a normal life now. I feel like a brand-new person.”
– Razel
“It would start off with an ache in my back or my legs, and then it would work its way down to my feet. Then it would go up to my arms, my neck and my head,” Razel says. “We’d try everything—hot showers, heating pads, pain medicine—but nothing worked. It would hurt so much that I couldn’t move. It felt like someone was crushing me with a dump truck.”
Razel suffered from these episodes, called pain crises, for most of his life. They happened once, twice, sometimes even three times a month, lasting for up to a week each time. Their cause: sickle cell disease, an inherited blood disorder wherein misshapen blood cells impede the vascular distribution of oxygen throughout the body, causing pain, organ damage and even stroke. Every time Razel had a crisis, it was as if his blood was suffocating him from the inside out.
“When you have sickle cell disease, you have a mutation in your beta-globin gene that causes your red blood cells to sickle—to be crescent-shaped instead of round,” explains pediatric hematologist/oncologist Alfred Gillio, M.D., director of the Children’s Cancer Institute at Joseph M. Sanzari Children’s Hospital at Hackensack University Medical Center. “These moon-shaped red blood cells get stuck in small blood vessels, which disrupts the flow of oxygen to tissue. It’s very painful.”
Historically, the only response to sickle cell disease was managing it with pain medication. Recently, however, new potentially curative treatments have emerged, including a cutting-edge gene therapy that has completely rid Razel of his condition and the paralyzing pain crises that accompany it.
A Challenged Childhood
Razel’s mother, Kyelia, knew something was different about her son. A few hours after delivering him via C-section, she held him for the first time and noticed his yellow pallor. He was jaundiced. Although he received phototherapy on the spot, it wasn’t until several days later that Kyelia and her husband, Felix, learned the cause of their baby boy’s turmeric-colored complexion.
“When we came home from the hospital, I asked my husband to get the mail. When he came back, there was a letter from the state, because when all children are born, the state requires them to get bloodwork [to screen for serious illnesses],” Kyelia recalls. “Before my husband even read the letter, he had this look on his face, and I said, ‘He has sickle cell disease.’ I don’t know how I knew. I just had a feeling.”
Sickle cell disease runs in Kyelia’s family. The inherited trait that causes it, however, is recessive. That means someone can carry the sickle cell trait but not actually have sickle cell disease. Babies only develop the disease if they inherit the trait from both of their parents. Although the trait is widely known to exist in African bloodlines, what’s lesser known is that it’s also present in Hispanic, Mediterranean and even Arab-Indian lineages. So while Kyelia, who is African American, knew she was a sickle cell carrier, her husband, who is Hispanic, had no idea that he was.
“Everyone always says sickle cell is an African American disease, so we were shocked,” Kyelia says.
Shock quickly became sorrow when baby Razel began exhibiting symptoms, the first of which was a high fever. When Kyelia rushed him to the nearest Emergency Department, she was referred to sickle cell specialists at a hospital 30 minutes away. Doctors there treated him with medication, but two and half months later, Razel was back in their nearest Emergency Department with yet another fever. Razel’s original hematologist was unavailable, but he sent a trusted colleague to help: pediatric hematologist/oncologist Stacey Rifkin-Zenenberg, D.O.
“When I first met Dr. Rifkin, I thought she was a superhero,” Kyelia says. “She came in an ambulance with a nurse and assessed Razel, then scooped him up and said to the EMT, ‘Let’s go. We’ve got to move.’ Then she whisked him out of there and took him to the hospital. That was the beginning of our relationship with Dr. Rifkin.”
Razel followed Dr. Rifkin-Zenenberg when she began practicing at Joseph M. Sanzari Children’s Hospital in 2016 as section chief for pediatric pain and palliative care. “I’ve known Razel since he was 3 months old,” Dr. Rifkin-Zenenberg says. “He’s gone through a lot in that time. He’s had a lot of hospital admissions and a lot of pain crises, and that’s impacted him dramatically.”
The impacts weren’t just physical. Because he was admitted to the hospital so frequently, Razel regularly missed school. And because sickle cell flares up when the body is under stress—from physical activity, infections or extreme temperatures—he was forced to abstain from normal childhood activities like sports, snowball fights and waterparks.
“My sickle cell disease got in the way of a lot of things,” says Razel, whose crises worsened when he reached adolescence, despite being on hydroxyurea, a chemotherapy drug that can reduce pain crises in sickle cell disease patients. “I couldn’t get in the sprinklers because the water was too cold for my body. I couldn’t even play outside with my friends because they would be running around and my body would start to ache if I tried to keep up with them. I’d feel pain, and I’d have to go back in the house and tell my mom. Next thing you know, we’d be on our way to the hospital.”
The End of Sickle Cell?
In the midst of so much pain, it would be easy to feel hopeless. But somehow, Razel remained unflinchingly optimistic.
“There were days when I thought, ‘I can’t deal with this,’ but I did because Razel didn’t complain,” Kyelia says. “He was in so much pain, but he would be the one comforting me. Even when he was hurting, he always told me, ‘Ma, don’t worry. I’m going to be healed from this.’ I didn’t understand how he could ever be healed from this—it was his blood—but he kept saying it.”
Adds Razel, “I just believed. There was no cure, but I always prayed they would come up with one.”
Today, there are two curative treatments for sickle cell disease. The first is a bone marrow transplant, which replaces a patient’s unhealthy blood-forming cells with healthy ones provided by a donor. This requires finding a well-matched (HLA-matched) bone marrow donor. Razel’s younger sister was not a match; siblings only have a 25 percent chance of being tissue-matched. A volunteer-matched donor or a half-matched donor can often be identified, although these alternative donor transplants can be associated with more complications.
Razel’s fortunes changed with the advent of a second therapy that’s currently undergoing clinical trials at sites across the country, including at Joseph M. Sanzari Children’s Hospital. Called LentiGlobin, it’s a gene-based therapy wherein doctors harvest the patient’s own stem cells and add to them a corrected gene that makes nonsickle hemoglobin. The patient then undergoes chemotherapy to kill off existing stem cells, after which the patient is transfused with their own genetically modified stem cells. Then the patient’s body can produce normal red blood cells that neutralize the effects of sickled red blood cells.
“Razel is the first patient in New Jersey to undergo this gene therapy trial,” says Dr. Rifkin-Zenenberg, the trial’s principal investigator at Joseph M. Sanzari Children’s Hospital. “And while I think it’s a little too early to say he’s cured, he’s been out of the hospital since December and hasn’t had any pain crises—and no evidence of sickle cell disease.”
If its curative effects hold, gene therapy could prove even more attractive than bone marrow transplants, says Dr. Gillio.
Gene therapy also surmounts graft-versus-host disease, a common transplant complication wherein immune cells in the donor’s marrow recognize that they’re in a foreign body and begin attacking the marrow recipient. Dr. Gillio adds, “Graft-versus-host disease can be significant and life-threatening, and when we use the patient’s own cells, we don’t have to worry about it.”
For Razel, what’s most exciting isn’t what’s happening in his cells, it’s what’s happening in his life: Without pain crises, he can go outside in the snow, swim, lift weights, go to the movies and even fly on airplanes—none of which he could do before. “I have a normal life now,” Razel says. “I feel like a brand-new person.”
Children with cancer need your help.  Your donation will save lives.
Your donation will save lives.